In a seemingly ordinary day in 1995, a 27-year-old construction worker in Leicestershire encountered an extraordinary twist of fate. While working at a building site, he jumped from a wooden plank, expecting to land on soft ground. Instead, he impaled his boot on a 15-centimetre nail protruding upwards. The immediate surge of agony was palpable, his body reacting as if serious injury had occurred. Rushed to the hospital, the casualty doctors administered fentanyl, a potent analgesic, followed by midazolam to manage his escalating distress before they dared to remove the nail. It was then that the truth emerged: the nail had threaded cleanly between his toes, leaving no physical injury. Despite the absence of any wound, his pain was undeniable, measured in elevated cortisol levels, increased blood pressure, and visible distress. This case, anonymised and later published in the British Medical Journal, starkly highlights a critical insight from pain neuroscience: pain is what the brain conjures when it believes the body has been damaged. The experience of pain is entirely real, even when the physical damage is not. This disjunction between damage and pain is more common than everyday assumptions suggest, challenging traditional models of how pain works.
The 1965 paper that started it
Before 1965, the scientific understanding of pain was deeply rooted in the ideas of René Descartes. In his 1664 work 'L'Homme', Descartes proposed a model where a fire under your foot would pull a string in the nerves, ringing a bell in the brain. This was the specificity theory, suggesting a direct line between the site of damage and the sensation of pain, with intensity directly correlating to the magnitude of the injury. For centuries, this 'private-line' concept dominated medical thought, treating pain as a passive, linear signal from the body to the brain.
The paradigm shifted dramatically in November 1965, when Ronald Melzack of McGill University and Patrick Wall of University College London published their groundbreaking paper in Science, 'Pain Mechanisms: A New Theory'. The gate-control theory they introduced posited that pain signals from the body pass through a metaphorical 'gate' in the spinal cord, specifically the substantia gelatinosa, before reaching the brain. This gate's modulation depends on competing signals from the body — the reason why rubbing a sore area can diminish pain — and descending controls from the brain, influenced by factors such as mood and attention. This model offered an explanation for the variability of pain perception with context and emotional state, igniting a revolution in pain research and treatment.
What the brain does

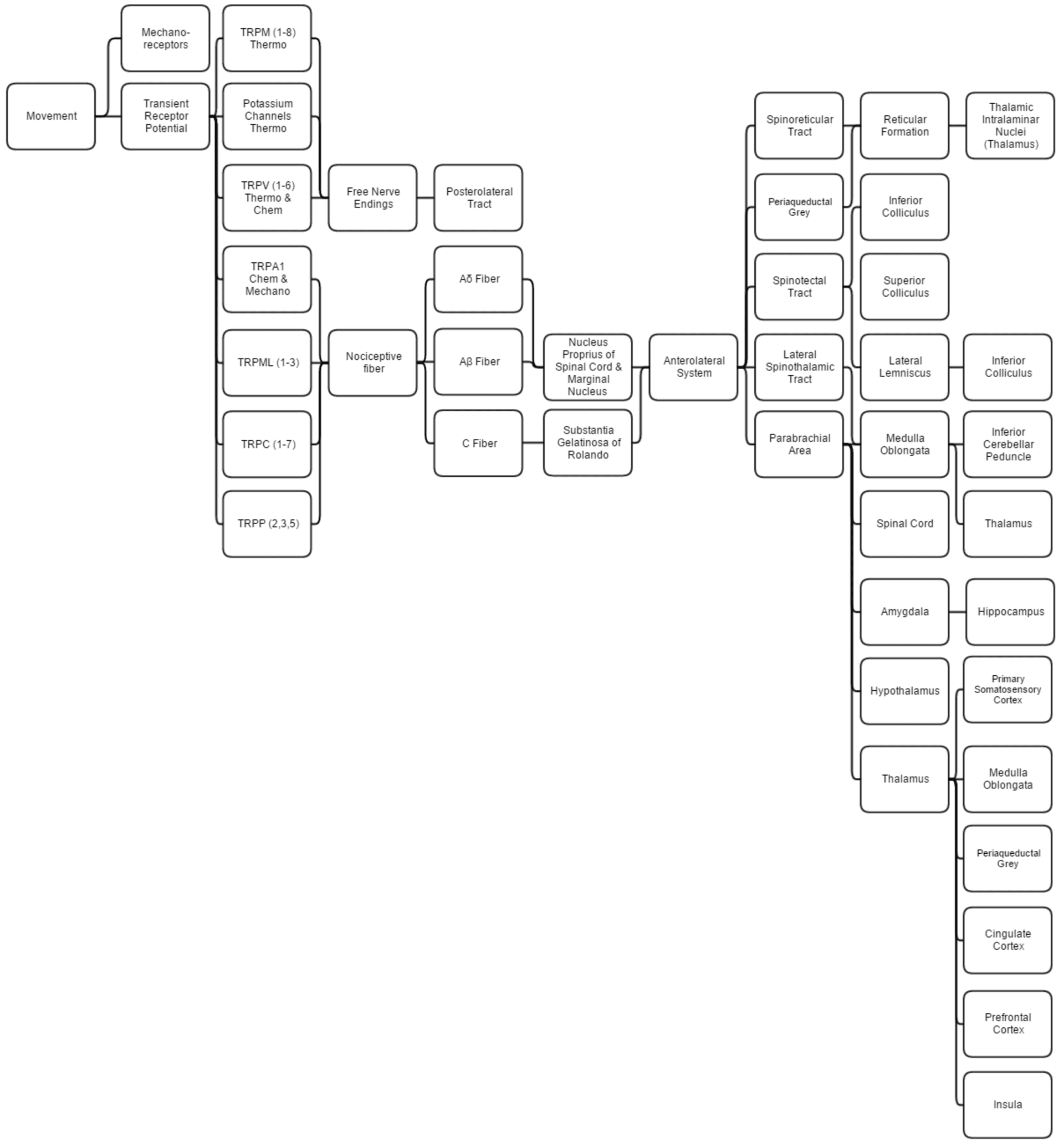
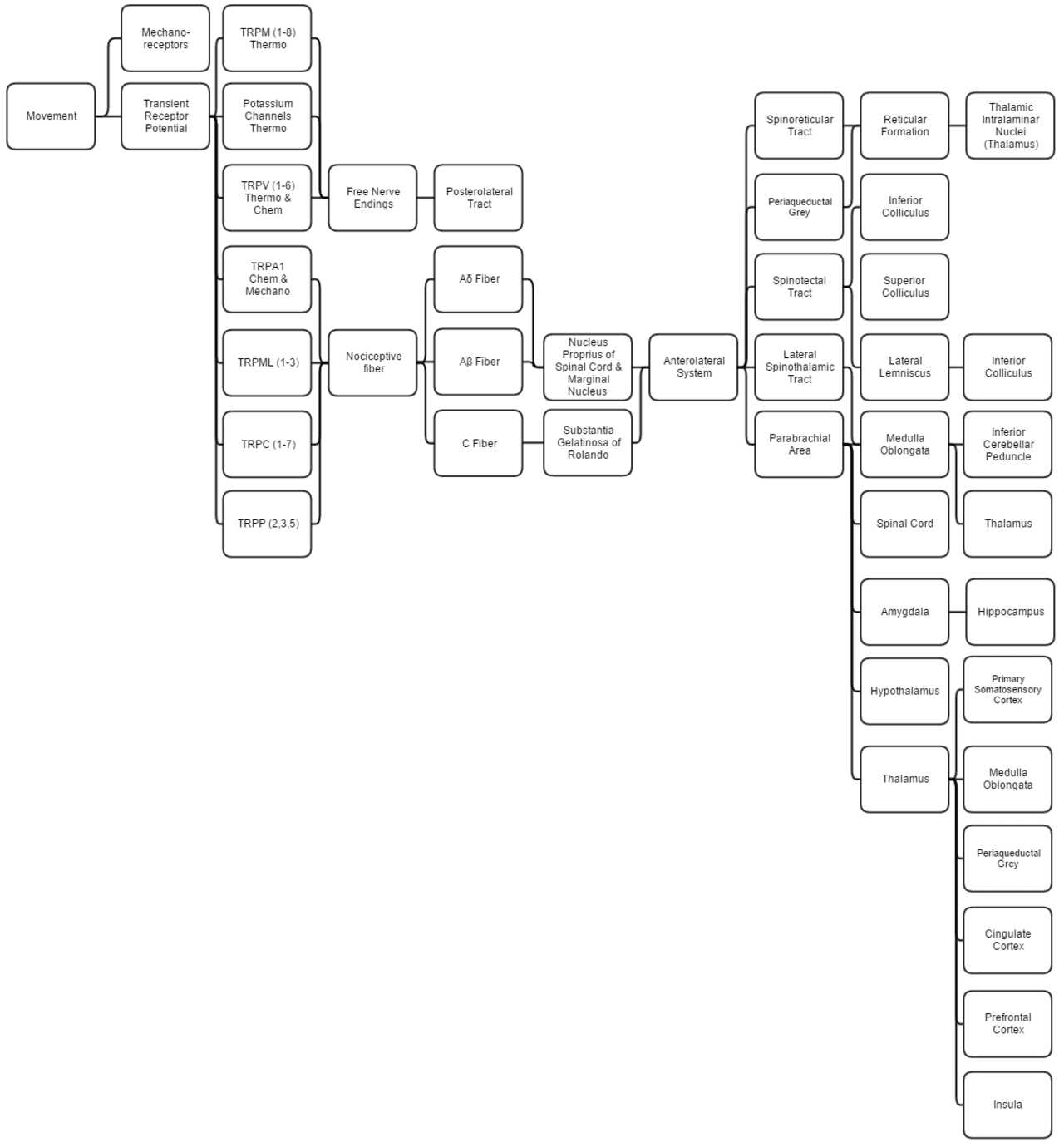
The developments in pain neuroscience since 1990 have refined the gate-control theory into a more complex understanding. Nociceptors, the specialised nerve endings, detect stimuli that could potentially cause damage — excessive heat, mechanical pressure, and certain chemicals. These nociceptors send their signals through two types of fibres: C-fibres, which carry slow, dull pain, and A-delta fibres, which convey fast, sharp pain. These signals reach the spinal cord, where the gate modulates them before they ascend to the brain.
Once in the brain, the signal is relayed by the thalamus to various regions: the somatosensory cortex localises the pain, the insula processes its visceral aspects, the anterior cingulate cortex deals with its emotional unpleasantness, and the prefrontal cortex is involved in interpreting its meaning. Pain, therefore, is not a direct transcription of injury but a conscious experience constructed from these inputs and influenced by expectations, past experiences, and current mental states. This network-based approach highlights that the same nociceptive input can result in different pain experiences depending on how the brain interprets these signals.
Why this matters for chronic pain
Acute pain serves a protective purpose: it prompts us to guard injured areas as they heal. Chronic pain, however, is a different entity. It persists long after the expected healing period, often in the absence of detectable injury, as seen in conditions like chronic back pain, fibromyalgia, complex regional pain syndrome, and neuropathic pain. In these cases, the gate-control model reveals its limitations because the problem is not ongoing tissue damage, but rather a maladaptive change in the pain-processing system itself.
Repeated nociceptive input can lead to 'central sensitisation', where the spinal cord and brain circuits responsible for processing pain become hypersensitive, amplifying signals that would previously have been innocuous. This adaptation, or rewiring, means that the system has effectively learned to react too strongly. The work of Lorimer Moseley and David Butler in the early 2000s highlighted how chronic pain is often about an overzealous protective response from the brain rather than continuing physical damage. This understanding shifts the treatment focus from addressing the tissue to recalibrating the brain's pain-processing mechanisms through education, graded activity, and psychological therapies.
The opioid problem
The late 20th century saw a sharp increase in the use of opioid medications to treat chronic pain, particularly in North America. The aggressive marketing of OxyContin by Purdue Pharma starting in 1996 played a pivotal role in this trend. By the mid-2010s, the United States was issuing opioid prescriptions at a rate of three per adult, fuelling an epidemic that would claim around 100,000 lives annually by the early 2020s. The logic underpinning this widespread prescribing was based on the outdated specificity model — the belief that pain directly equated to damage and that opioids, by blocking pain signals, were therefore addressing the root cause.
However, the advancements in pain science have shown why this rationale was flawed. Opioids are effective for acute pain as they dampen the nociceptive input, but in chronic pain, their efficacy diminishes rapidly. The body adapts to the drug, requiring higher doses for the same effect, while the underlying issues of central sensitisation remain unaddressed. Opioid-induced hyperalgesia, where prolonged opioid use leads to increased pain sensitivity, further complicates treatment. The opioid epidemic starkly illustrates the consequences of applying a 17th-century understanding of pain to a problem that demands a contemporary, nuanced approach.
What works instead
In response to the limitations of opioid treatments, modern pain management has embraced approaches that address the brain's role in pain. Pain neuroscience education (PNE), pioneered by Adriaan Louw and others, involves educating chronic pain patients about how the brain processes pain. Even a brief 30-minute conversation about the overprotective nature of the pain system can significantly reduce pain perception. The patient's understanding of pain as a brain construct, rather than a direct consequence of tissue damage, can transform their experience.
Graded exposure to movement, an approach championed by Lorimer Moseley, helps retrain the pain system to tolerate previously painful activities. Cognitive Behavioural Therapy (CBT), including Kabat-Zinn's mindfulness-based stress reduction techniques, targets the psychological aspects that exacerbate pain, such as catastrophising and hypervigilance. Pharmacological treatments have also evolved, with low-dose tricyclic antidepressants and anticonvulsants being used to modulate pain pathways without inducing dependence. Additionally, peripheral nerve treatments like capsaicin patches and certain neurostimulators offer relief by acting on the original input rather than the pain network. This multi-faceted approach — combining education, movement, cognitive therapies, and targeted medication — consistently outperforms opioid therapy in treating chronic pain.
What is still hard
Despite significant advancements, many challenges remain in the field of pain research. Acute postoperative pain is often inadequately managed, particularly in children, the elderly, and non-verbal patients. Cancer pain continues to be a domain where opioids have a necessary and justified role. Phantom-limb pain, a condition where individuals experience pain in a limb that no longer exists, underscores the extent to which pain is a construction of the brain, and yet it remains stubbornly resistant to treatment.
The genetic basis for pain sensitivity, as highlighted by variations in the SCN9A gene, is still being explored, with some people exhibiting extreme sensitivity while others have congenital insensitivity to pain. These genetic factors add another layer of complexity to pain management. Additionally, ethical considerations in animal research on pain, which seeks to minimise suffering while achieving scientific insights, continue to pose dilemmas. While the framework for understanding and treating pain has evolved considerably since 1965, the practical application lags behind, with a wide gap between research findings and clinical practice in many healthcare systems.
Pain is undeniably real. It is a construct of the brain, responding to a myriad of inputs, some of which include tissue damage. Pain can persist even after tissues have healed because the neural system responsible for interpreting pain may have changed. Treatments for chronic pain that focus on retraining the brain's pain-processing mechanisms are more effective than those targeting the tissue alone. The construction worker who believed a nail had penetrated his foot experienced genuine pain due to a perceived threat. His case exemplifies the current understanding: pain is the brain's response to its assessment of potential damage, irrespective of actual harm. This model not only provides a more compassionate view of pain but also offers practical solutions that validate the patient's experience and improve treatment outcomes. As the field progresses, the insights gained since Melzack and Wall's 1965 paper will continue to inform and refine our approach to one of the most fundamental human experiences.
References
- Melzack, R., & Wall, P. D. (1965). Pain mechanisms: a new theory. Science, 150(3699), 971–979.
- Moseley, G. L., & Butler, D. S. (2017). Explain Pain Supercharged. Noigroup Publications.
- Fisher, J. P., Hassan, D. T., & O'Connor, N. (1995). Minerva. British Medical Journal, 310, 70.
- Loeser, J. D., & Treede, R.-D. (2008). The Kyoto protocol of IASP Basic Pain Terminology. Pain, 137(3), 473–477.


